INFORCE™ Biopsy: One-Step Method for Incision and Forceps Biopsy Procedure During Endoscopy
Sector
Gastrointestinal endoscopy biopsy
Development Phase
Preclinical
Description
Physicians at Tufts Medical Center have invented a device that allows incision and forceps biopsy to be performed as a one-step procedure with a single instrument rather than with two distinct catheters.
Problem
Subepithelial lesions are a common finding during upper endoscopy (EGD). Of the more than 2.8 million EGDs performed in the United States annually, there is an estimated 3.5% incidence of subepithelial tumors, with a total of 98,000 patients who require evaluation. Tissue sampling of the subepithelial lesion is essential to establish the diagnosis, which may include GI stromal tumors, malignant lymphomas, carcinoid tumors, gastric cancer, and benign tumors such as leiomyomas, aberrant pancreas, and lipomas. Current tools for biopsy of upper GI subepithelial lesions are awkward and offer poor diagnostic yield (17-65%).
Lead Investigator(s)
Moises Guelrud and Keo Thormika, Department of Medicine, Gastroenterology, Tufts Medical Center, Boston, Massachusetts
Contact
Nancy Wetherbee
NWetherbee@tuftsmedicalcenter.org
617 636 6182
Current Technology
The 98,000 patients requiring evaluation are currently managed with serial EGD surveillance and endoscopic ultrasound with fine-needle aspiration. EUS-FNA has an average diagnostic yield of 45%, with the procedural limitations that it requires an on-site cytopathologist and is appropriate for lesions of larger than 20 mm. Another technique is endoscopic ultrasound (EUS) with single-incision needle-knife (SINK) biopsy, which can be performed on lesions smaller than 20 mm and has a low risk of complications. After EUS examination of the subepithelial lesion, a 6 to 10 mm linear incision is made with a needle-knife sphincterotome, followed by introduction of large-capacity biopsy forceps for obtaining tissue specimens and closing the incision with endoclips. Although the SINK technique has a 92% diagnostic yield, it involves the use of two distinct catheters and occlusion clip placement, and it is expensive.
Solution
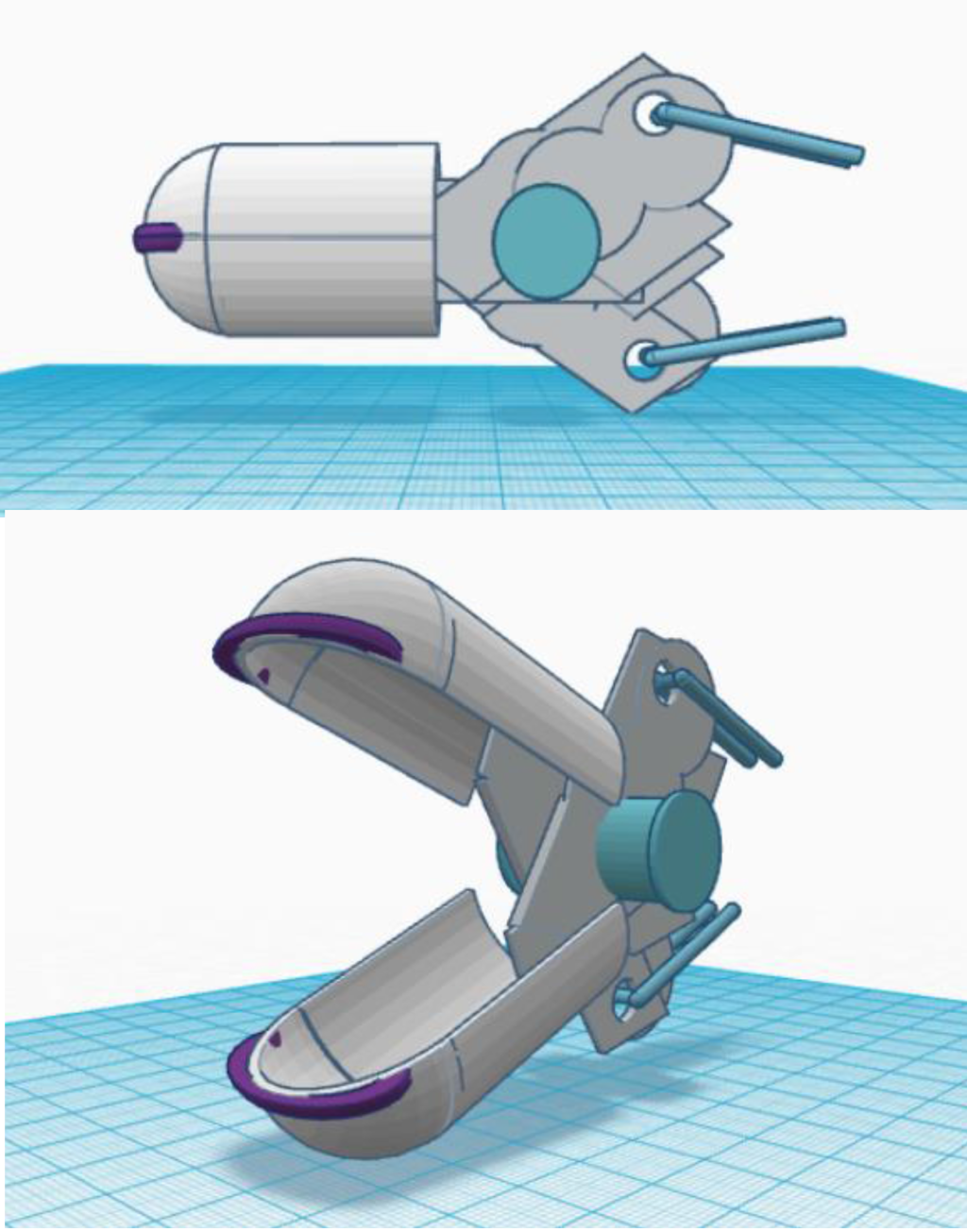
Tufts Medical Center physicians have invented a device that allows incision and forceps biopsy to be performed as a one-step procedure with a single instrument rather than with two distinct catheters. The invention is inserted through the endoscope working channel as a standard biopsy forceps. The unique design features of Tufts Medical Center’s INFORCE™ biopsy device mitigate the risk of perforation with a blunted forceps edge, which improves the margin of safety of performing subepithelial biopsy in comparison with available tools.
INFORCE™ Biopsy Device for Performing Incision Biopsy
Some operators may avoid performing SINK biopsy because of reluctance to using a needle-knife sphinctertome. Tufts Medical Center’s INFORCE™ biopsy device has several innovative features that address the particular operator requirements of the SINK technique and that supplement “hot biopsy forceps” designs on the market. The INFORCE™ biopsy solution would require modest incremental demands to translate into a commercial product.